Medicaid was passed as part of the Social Security Amendments of 1965 (Medicare was Title 18 and Medicaid was Title 19 entitled “Grants to the States for Programs of Medical Assistance”) and signed by President Johnson as part of his Great Society legislative agenda. While President Teddy Roosevelt thought about national health insurance in some form as early as 1908, President Franklin Roosevelt included it his New Deal legislative agenda during the Great Depression. However, after fierce opposition by the American Medical Association (their concern was that insurance would undermine physician autonomy), national health insurance was pulled from the Social Security Act of 1935 in order to save the federal retirement program (Social Security). According to David Smith (Entitlement Politics: Medicare and Medicaid), 30 years of state and federal public assistance programs followed with limited financial assistance for medical care through either direct (cash) or vendor payments. Medicaid’s original eligibility criteria was limited to the following categories: families with dependent children (typically single-parent), the elderly, the blind, and the disabled. Those who were eligible also had to meet income and resource requirements called means testing. States were responsible for eligibility determination beyond the federal minimums under the definition of “medically needy” and the administration of the program in the state. Federal matching support for Medicaid varied in each state ranging from 83 percent in poor states to 50 percent in wealthier states based on the state’s per capita income.
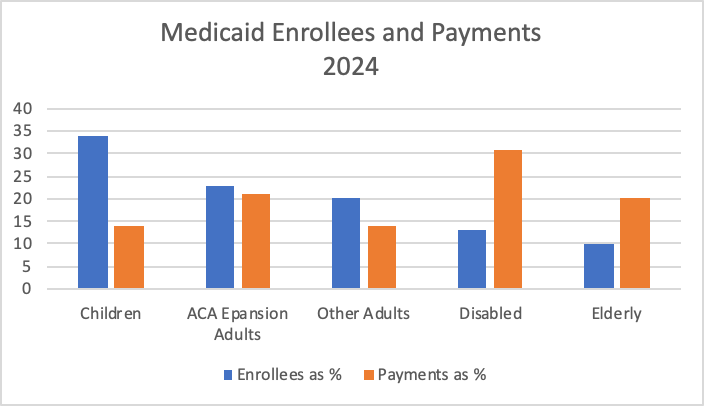
Two issues were apparent concerning Medicaid from the very beginning. The first was to expand eligibility and benefits like expanding eligibility to pregnant mothers and nursing home residents and expanding benefits including preventive care and post-hospital care. The second was controlling the cost which increased from $5.3 billion in 1970 to $931.7 billion in 2024. Where Medicaid money goes can be surprising. For instance, while disabled and the elderly represent 23 percent of Medicaid enrollees, those two groups account for over 51% of payments.
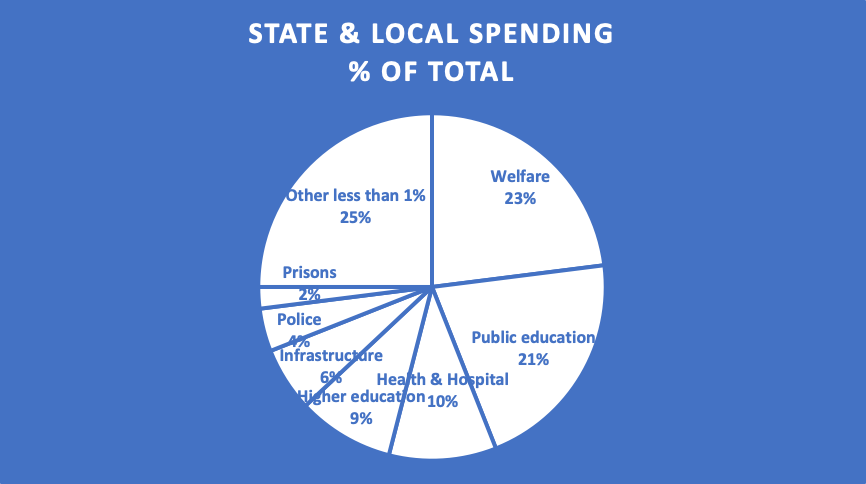
The Urban Institute (2021) has analyzed the impact of Medicaid spending on state and local budgets. The largest components of state and local budgets in the 1970’s included education, higher education, infrastructure (roads and bridges), and correctional facilities. Today, welfare spending including Medicaid is the largest expenditure in virtually every state (Medicaid spending is part of welfare spending and part of health and hospital spending—Medicaid spending is 27 percent of state and local spending. It is important to note that states do not absorb all of the increase in spending. For instance, much of the increase in Medicaid spending has been passed on to the federal government via formula funding and much of the increase in higher education has been passed off to college students in the form of higher tuition and fees. However, there is little doubt that increasing Medicaid spending has impacted other state and local spending (welfare spending including Medicaid spending has increased 485 percent since 1977 after adjusting for inflation).
An exhaustive review of Medicaid legislation is outside the purview of this blog, but can be found in Smith’s Entitlement Politics or in my book Introduction to the Financial Management of Health Care Organizations. However, a review of fraud and abuse definitions is instructive.
- Fraud is the intentional act of deception or misrepresentation that results in some form of benefit to the actor. Fraud is a criminal act and can result in incarceration.
- Abuse refers to provider practices that do not follow accepted business or medical practices and result to unnecessary cost to the Medicaid program. Abuse is generally a civil act resulting in fines.
- Waste is the inappropriate utilization of services that result in unnecessary cost to providers.
- Errors are mistakes made without intent or knowledge of the error.
- Improper payments are Medicaid payments to providers that should not have occurred. Improper payments are generally not fraud unless government can prove intent or a pattern of deceit. The improper payment rate in Medicaid is 5.1 percent representing $31 billion in improper payments recovered by Medicaid.
CMS provides a detailed report of Medicaid (and Medicare) fraud, abuse, and waster to Congress (see https://www.cms.gov/files/document/fy2024-medicare-medicaid-report-congress.pdf)